When a practice administrator posts a job for “triage nurse,” the title gets applied loosely. It covers everyone from call-routing clerks to advice line staff to seasoned RNs running physician-approved protocols. Those differences carry real clinical and legal weight.\ \ Triage nurse meaning comes down to a specific role. It describes a registered nurse who combines structured, evidence-based protocols with professional clinical judgment. The goal is to determine the safest, most appropriate level of care for each patient.
The wrong coverage model can leave patients without proper guidance. It can also expose organizations to real risk. A model that looks like triage but lacks the clinical foundation is not triage. The right model is built on trained RNs, validated protocols, and clear escalation pathways.
That is what separates genuine nurse triage from administrative call handling dressed up with a clinical title.
The Word and the Work
The word triage comes from the French verb trier, meaning “to sort.” That etymology still explains the job precisely. A triage nurse sorts patients by clinical urgency. Arrival order and caller persistence are irrelevant. The clinical picture is what drives every decision.
A triage nurse is a registered nurse who serves as the first clinical touchpoint for patients. She applies critical thinking and evidence-based protocols to assess symptoms. Her job is to direct people to the right care setting. That is a fundamentally different role from a scheduling coordinator or a general advice nurse.
Urgency assessment, risk stratification, and disposition guidance form the core of the work. These tasks demand the training and licensure that an RN credential carries. Professional nursing organizations consistently hold that this role requires an RN at minimum. A medical assistant or front-desk staff member cannot step in, regardless of experience in other tasks.
Telephone triage is the fastest-growing expression of this function. Nurses conduct the same structured clinical assessment by phone, following physician-approved protocols like Schmitt-Thompson to guide every decision. No physical exam is possible. That constraint makes the nurse’s ability to listen, probe, and interpret even more critical.
Our nurse triage handbook covers the clinical scope and operational standards that define the role across both settings.
Three Decisions in Every Call
Every triage encounter comes down to three questions: How urgent is this? What level of care fits? How quickly does the patient need to move? Those questions apply whether the encounter happens in a hospital hallway or over a phone line.
The workflow follows a clear sequence. The nurse gathers a structured symptom history using approved clinical tools. She then assesses what the presentation actually suggests and directs the caller to the appropriate care setting. Our nurses follow physician-approved Schmitt-Thompson protocols as the clinical backbone of every call.
Each assessment is consistent, defensible, and grounded in evidence rather than intuition alone. That standard matters when outcomes are audited.
Consider a caller reporting chest tightness in a 58-year-old. A simple call-routing script stops at the symptom. A trained triage RN asks follow-up questions. She surfaces the fact that the tightness started on exertion and is now accompanied by diaphoresis.
The call ends with a 911 recommendation, not a next-day appointment.
No script produces that outcome.
The nurse’s role in every call covers three linked steps:
- Gather: Structured symptom questioning in a protocol-defined order. Onset, severity, associated symptoms, and relevant history are each addressed.
- Assess: Applying Schmitt-Thompson protocol logic alongside clinical experience. The goal is to distinguish a routine complaint from a presentation that warrants escalation.
- Direct: Assigning a care disposition. Options range from self-care at home to urgent care to an immediate 911 recommendation.
Routing is the output, not diagnosing or treating. Every decision stays within the nurse’s scope of practice. Some callers downplay symptoms, others struggle to describe pain, and some are calling about someone else entirely. A nurse’s training accounts for all of it.
Nurse Triage vs. Telemedicine vs. Symptom Checkers
Telephone nurse triage and telemedicine are often grouped together. They carry different clinical scopes, liability profiles, and staffing requirements. Conflating them is not just a semantic error. It can expose your organization to scope-of-practice risk and protocol gaps that regulators and payers will notice.
A triage nurse assesses symptoms and routes the patient. She applies evidence-based protocols and does not diagnose. A telemedicine provider, typically a physician or nurse practitioner, delivers a remote diagnosis and may prescribe treatment. These are fundamentally different clinical acts, governed by different licensing standards, with different billing codes.
A third category complicates the picture further: AI-driven symptom checkers. These tools can surface a list of possible conditions, but they carry no licensed clinical judgment. A symptom checker cannot hear the catch in a caller’s voice. It cannot notice that a parent’s answers are growing vaguer and more frightened.
A trained triage RN can do all of that. Clinical judgment cannot be automated. AI cannot hear fear in a parent’s voice. Technology supports the process, but clinical judgment drives every decision.
That accountability layer is a structural requirement, not a soft advantage.
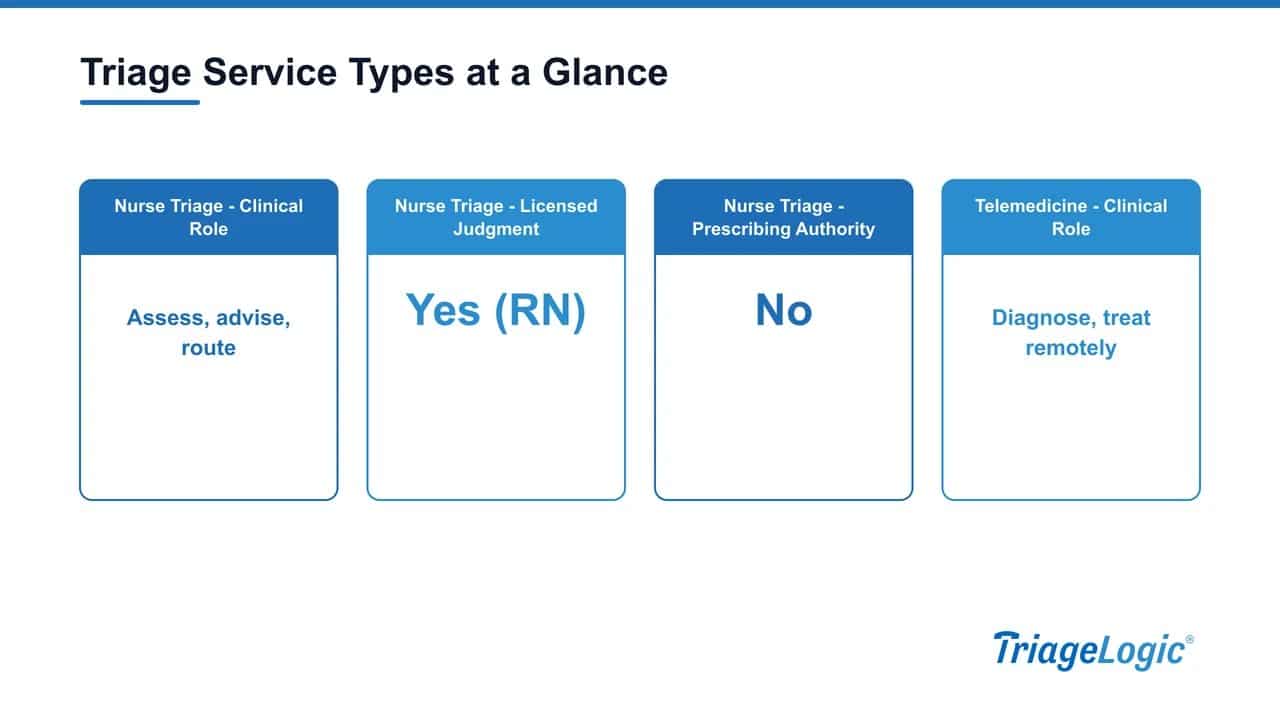
The table below compares each service type across three dimensions:
| Service Type | Clinical Role | Licensed Judgment | Prescribing Authority |
|---|---|---|---|
| Nurse Triage | Assess, advise, route | Yes (RN) | No |
| Telemedicine | Diagnose, treat remotely | Yes (MD/NP/PA) | Yes |
| Symptom Checker | Surface possible conditions | No | No |
Our guide on how to assess whether a vendor’s clinical model meets triage standards walks through the questions worth asking before you sign a contract.
The Protocol Standard: Why Schmitt-Thompson Is the Benchmark
Schmitt-Thompson protocols are used in the vast majority of medical triage call centers across North America. They handle an enormous volume of calls per year. That scale makes them the closest thing the industry has to a universal clinical standard. Asking whether nurses follow protocols is only a starting point.
The more precise questions are: which protocols, how current are they, and who approved them?
Schmitt-Thompson guidelines are evidence-based. A peer panel reviews them annually. Each protocol is organized by symptom. That structure gives every triage nurse a reproducible decision tree to follow.
Clinical override remains available when the situation calls for it. That detail matters. A printed protocol cannot hear a parent’s voice crack with fear. Clinical judgment grounded in structured guidance is what separates a trained RN from a static decision flowchart.
TriageLogic has operated on that foundation since 2006. Want a closer look at nurse triage protocols and how they protect clinical consistency? Our dedicated guide covers what administrators should verify before signing any service agreement.
The Stakes: What Happens When Coverage Doesn’t Clear the Bar
Roughly 24% of ER visits among working-age adults are for non-urgent reasons, according to a 2024 NCQA study. A significant portion of those visits trace back to a failed or missing triage step. That is not a patient education problem. It is a coverage gap.
The financial weight is real. A 2020 study cited by NCQA put aggregate U.S. emergency room costs at $76.3 billion, with misdirected, non-urgent visits baked into that number. When a patient cannot reach a qualified clinical voice after hours, the ER becomes the default. Not because it is the right level of care.
Because it is the only door that stays open.
Research supports the value of closing that gap. One peer-reviewed study published on PMC/NCBI examined an after-hours nurse line and found that 70% of calls were resolved without physician involvement. None of the patients directed to home care subsequently needed an ER visit or hospitalization.
Our own data shows approximately 1 in 6 triage calls prevents an unnecessary ER visit. Every call handled well is also a cost avoided. Our data on patient symptom calls and care outcomes from nurse triage illustrates what closing that gap looks like in practice.
The after-hours window is where the gap bites hardest. According to a KLAS report published by the American Hospital Association, 45% of physicians cite after-hours workload as a burnout contributor. Inadequate coverage falls on staff as well as patients.
Accreditation: What It Covers and How to Verify It
URAC Health Contact Center (HCC) accreditation is the independent quality credential that matters most here. It separates a credentialed nurse triage operation from a vendor that simply employs nurses. The standard sets documented requirements across clinical protocols, callback response times, staff qualifications, and quality assurance processes. Periodic external review is required to maintain it.
This is distinct from URAC’s separate Telehealth accreditation program. The two are not interchangeable.
URAC HCC accreditation reflects accountability in measurable terms. Our nurses return calls in about 9 minutes on average, well within the URAC 30-minute benchmark. The physician-led network behind our service includes more than 22,000 physicians and covers over 42.5 million lives. Clinical oversight scales with call volume rather than straining under it.
You can explore how outsourced after-hours nurse triage and coverage models work to understand what that infrastructure looks like in practice.
When evaluating any vendor, ask for specifics, not promises. Request documentation across five areas:
- Accreditation certificate: Request the current URAC HCC certificate. Confirm the expiration date directly with URAC.
- Callback time data: Ask for documented average callback times, not just a stated target.
- Protocol documentation: Confirm nurses follow physician-approved clinical protocols such as Schmitt-Thompson, not internal guidelines built without clinical validation.
- QA audit cadence: Ask how often call quality is reviewed, by whom, and what happens when a call falls outside protocol.
- Staff qualification standards: Verify RN licensure requirements and any ongoing competency training.
Nurse triage handles calls that require clinical judgment. Routine front-desk volume is a separate problem that deserves a separate solution. Our automated patient message-intake product, MedMessage Automate, captures structured patient requests 24/7 through physician-designed secure-text pathways. It shifts roughly 65% of routine front-desk calls to text and saves 3 to 7 minutes per message.
Nurses stay focused on the calls that actually need them.
Frequently Asked Questions
What is the difference between a triage nurse and a regular staff nurse?
A triage nurse’s primary function is assessment and care routing. The role involves determining urgency and directing the patient to the right level of care, not delivering hands-on or ongoing treatment. It requires strong clinical judgment, structured protocol use, and the ability to make rapid dispositions with limited physical assessment cues.
Do telephone triage nurses diagnose patients?
No. Telephone triage nurses assess symptoms and direct patients to the appropriate care setting. They do not diagnose or prescribe. Diagnosis and treatment fall within the scope of telemedicine, which involves a licensed physician or advanced provider.
What protocols do outsourced triage nurses use?
The industry standard is Schmitt-Thompson clinical protocols, used in more than 95% of North American medical triage call centers. Any outsourced triage vendor should be able to confirm which protocol set their nurses follow, the version in use, and who provides physician oversight for protocol approval.
How fast should a triage nurse return a patient call?
URAC’s Health Contact Center accreditation sets a 30-minute benchmark for callbacks. Administrators should request documented average callback time data from any vendor under evaluation, not just a stated target.
Can outsourced nurse triage actually reduce unnecessary ER visits?
Yes. Research supports it at multiple levels. One peer-reviewed study published on PMC/NCBI of an after-hours nurse line found 70% of calls resolved without physician involvement. None of the patients directed to home care subsequently needed an ER visit or hospitalization.
Our internal data shows approximately 1 in 6 triage calls prevents an unnecessary ER visit. A 2024 NCQA study confirms that roughly 24% of working-age adult ER visits are non-urgent, which means well-designed triage can redirect a meaningful share of that volume.
Closing Thoughts
Nurse triage is a clinical quality layer, not a staffing convenience. When coverage falls short, real patients face real consequences: calls go to voicemail, unlicensed staff make disposition decisions, and no structured protocol guides the conversation.
Administrators who understand what the role requires are better positioned to assess their current model honestly. That means knowing which accreditation standards apply, what physician-led oversight looks like, and where the gaps are.
TriageLogic holds URAC Health Contact Center accreditation, follows Schmitt-Thompson clinical protocols, and our physician-led network spans more than 22,000 physicians covering over 42.5 million lives. Want to see what that combination of credentialed process and clinical oversight looks like in practice? The Nurse Triage Protocols guide is a practical starting point for any team reviewing their after-hours coverage.
Medically reviewed by a TriageLogic clinical professional.