After Hours Medical Answering Service: What RN Triage Actually Does (and Why It Matters)
By TriageLogic
A parent calls your clinic at 1 a.m. Her toddler has a fever of 104 and she’s scared. A traditional answering service takes a message and promises a callback.
An after-hours medical answering service staffed by registered nurses puts a clinician on the line within minutes. That nurse works through physician-approved Schmitt-Thompson protocols. Together, the nurse and parent decide: does this situation call for an ER trip, or careful home monitoring? That distinction – message relay versus clinical judgment – is the entire argument.
For healthcare organizations weighing after-hours coverage options, the difference is not cosmetic. One approach documents a call. The other resolves it. Structured clinical reasoning protects patients and reduces unnecessary ER visits. It also shields physicians from overnight calls a trained nurse can handle safely.
Message Relay vs. Clinical Triage: A Patient Safety Issue
A traditional medical answering service routes calls and logs messages. An RN-staffed after-hours triage service evaluates symptoms promptly, assigns acuity, and routes patients to the right level of care.
Consider what happens when a parent calls about a child with a high fever and labored breathing. A staff member logs the call. A nurse or on-call physician eventually gets a message sometimes a late as the next day. No one assesses whether that child needs an ambulance in ten minutes or whether a cool cloth and a morning appointment would do. That clinical gap carries real consequences.
According to research published in After-Hours Care and its Coordination with Primary Care in the U.S., only 29% of U.S. physicians reported having arrangements for true after-hours care beyond an automated ER referral. The vast majority of patients have no access to real clinical guidance after hours.
The outcome is predictable. Nearly 65% of all ER visits occur between 5 p.m. and 8 a.m. or on weekends. Primary care offices close during those hours. A service that only takes messages cannot interrupt that pattern. A registered nurse following Schmitt-Thompson protocols can.
Here is the flow that separates a clinical triage call from a message relay:
- Symptom evaluation in real time: All calls are first answered by a non-clinical operator. The calls are then added to a call queue and a nurse returns the call based on acuity (more urgent calls are addressed first) with the average call
- Acuity assignment determines the right level of care – an ER, urgent care, a next-day appointment, or home management guidance.
- Protocol-driven consistency means every caller receives care guided by the same physician-approved Schmitt-Thompson clinical standards.
- Documented clinical encounters integrate with existing workflows, not a phone log sitting in a queue.
- Appropriate ER diversion for non-urgent concerns protects both the patient’s time and the ER’s capacity for genuinely emergent cases.
Your team may be weighing these options right now. Download the guide to after-hours nurse triage on call for a side-by-side look at how the two models differ, covering both clinical outcomes and operational cost.
The Cost of the After-Hours Gap: ER Overuse, Burnout, and Staffing Shortages
Three pressures are pushing health systems toward outsourced after-hours triage: unnecessary ER visits, physician burnout, and an RN workforce shortage. Each one makes in-house staffing harder, and each pressure compounds the others.
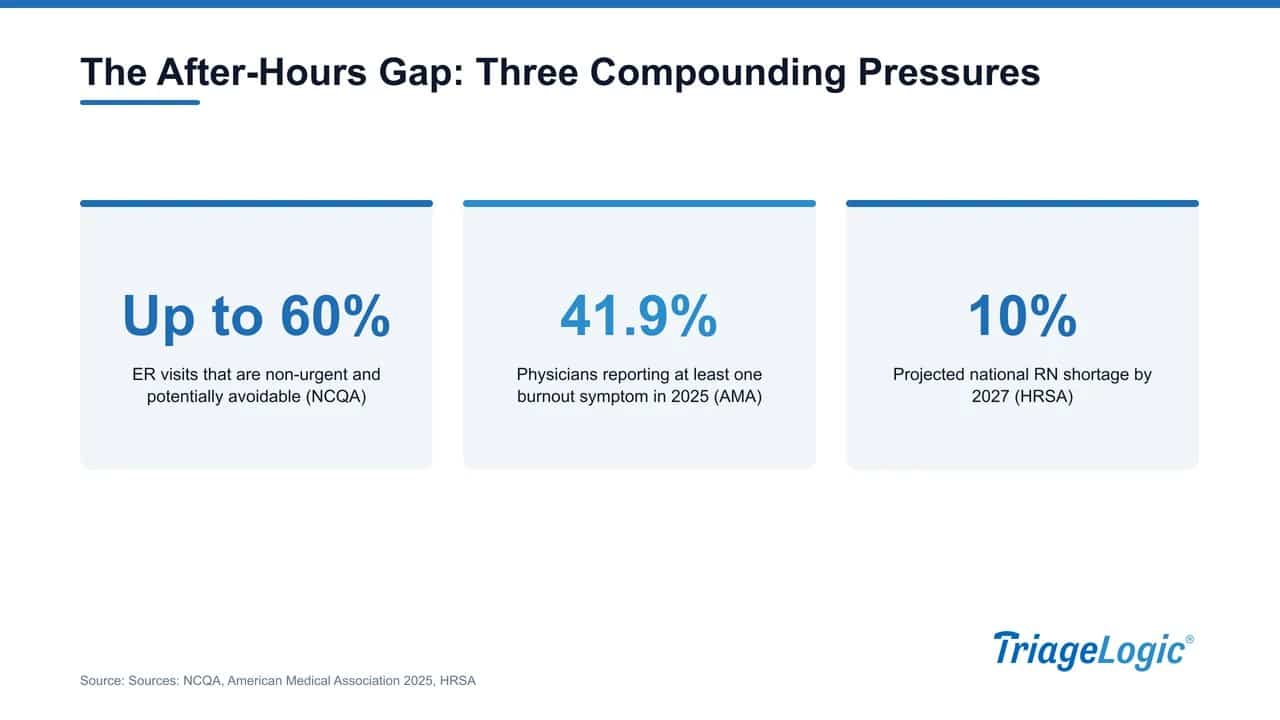
According to NCQA, up to 60% of all ER visits are non-urgent and potentially avoidable. That overcrowding delays care for patients who genuinely need emergency attention. A trained RN following Schmitt-Thompson protocols can redirect low-acuity callers in real time. A recorded message cannot.
The American Medical Association found that 41.9% of physicians reported at least one burnout symptom in 2025. After-hours call burden is a well-documented contributor. Removing overnight and weekend calls from a physician’s schedule reduces one of the most disruptive pressures they face.
Staffing closes the trap. HRSA projects a 10% national RN shortage as early as 2027. Outsourcing solves the staffing equation without requiring recruitment, training, or round-the-clock scheduling of clinical staff.
Our guide to evaluating a medical call center vendor walks through what to look for when comparing options.
| Pressure Point | Scale of the Problem | How Outsourced RN Triage Helps |
|---|---|---|
| Unnecessary ER visits | Up to 60% of ER visits are non-urgent (NCQA) | Clinical triage redirects low-acuity callers to appropriate care settings |
| Physician burnout | 41.9% reported burnout symptoms in 2025 (AMA) | Removes after-hours call burden from on-call physicians and office staff |
| RN workforce shortage | 10% national shortage projected by 2027 (HRSA) | Outsourced staffing eliminates the need to recruit and retain in-house triage nurses |
How a Nurse Triage Call Actually Works
When a patient calls after hours, a licensed RN answers and works through Schmitt-Thompson clinical protocols to assign an acuity level. The nurse then decides the right next step: some calls close with phone guidance, others route to a next-day appointment, an on-call provider, or the ER.

Our nurses complete that process in about 9 minutes on average – well within the URAC 30-minute benchmark for health contact centers.
According to a systematic review published in The Effects of Telephone Consultation and Triage on Healthcare Use and Patient Satisfaction, at least 50% of after-hours calls resolve by phone alone, with no in-person visit required. Our own data shows roughly 1 in 6 triage calls avoids an unnecessary ER visit.
For a detailed look at how these protocols work in practice, download the guide to nurse triage protocols.
Here is what happens at each stage:
- Call receipt: initial intake goes to answering service, then a licensed RN calls back within 30 mins. (TriageLogic’s team averages 9 minutes) No extended hold queue, no automated menu.
- Protocol engagement: The nurse opens the relevant Schmitt-Thompson pathway and works through structured clinical questions.
- Acuity assignment: The nurse maps symptoms to a disposition level, ranging from home care advice to immediate ER referral.
- Resolution or escalation: Most calls close with phone guidance or a next-day appointment; urgent cases route to the on-call provider or ER with documented clinical rationale.
- Documentation: The encounter is recorded for continuity of care, giving the primary team a clear picture of what happened overnight.
Why URAC Accreditation Is Non-Negotiable
URAC Health Contact Center accreditation signals that a service meets defined standards for clinical staff qualifications, response times, HIPAA-compliant documentation, and ongoing quality assurance. It is not a marketing badge. For enterprise buyers, it is a structural requirement.
URAC’s accreditation includes a Clinical Contact Center Module specifically for organizations performing health triage, with measurable thresholds: nurse qualifications, telephone performance standards, call-handling protocols, and auditable documentation practices.
A vendor claiming general HIPAA compliance is not the same as a vendor whose triage workflows have been reviewed and verified against those standards. That difference matters when a CMO is signing an outsourced contract. Consider what a compliance gap looks like in practice: a health system partners with a triage vendor that lacks accreditation, a payer audit surfaces, and the health system cannot demonstrate that call-handling met any defined clinical standard.
Credentialing is not overhead. It is protection.
We are URAC-accredited, physician-led, and founded in 2006. Our nurses follow physician-approved Nurse Triage On Call with Schmitt-Thompson protocols, every call generates auditable logs your compliance team can review, and continuous nurse training is built into operations rather than treated as a one-time credentialing event.
Scale, Specialty Coverage, and What We Bring to the Table
Our physician-led network includes more than 22,000 physicians and covers over 42.5 million lives. That scale eliminates the single-point-of-failure risk that plagues smaller, in-house arrangements. When one nurse calls in sick, our network absorbs that variability without disruption.
Specialty depth matters as much as scale. Our nurses follow Schmitt-Thompson clinical protocols across pediatrics, OB/GYN, cardiology, primary care, and FQHCs, among others.
Multl-lingual triage support means a worried parent calling at 1 a.m. can describe symptoms in the language they think in. The nurse hears the full picture and makes an informed clinical decision. A trained nurse can also hear hesitation, fear, or the quiet urgency a caller is trying to minimize. Technology supports the process; clinical judgment drives every decision. That philosophy shapes our TriageLogic after-hours medical answering service, where registered nurses handle calls according to evidence-based protocols rather than scripted decision trees.
For operations leads, EHR integration matters too. Our platform documents triage encounters and passes structured data back into your existing workflows, reducing documentation burden without adding another disconnected system.
Outsourced Triage vs. In-House On-Call: How to Think About the Decision
Comparing outsourced and In-House On-Call after-hours coverage comes down to four factors: clinical quality, cost predictability, staff burden, and scalability.
An In-House On-Call model carries unpredictable overtime, liability exposure, and the administrative weight of scheduling coverage gaps. An outsourced After Hours Medical Answering Service replaces that variability with a defined per-call or monthly cost structure, making budgeting far more predictable.
Staff burden is harder to quantify but equally important. After-hours calls are a documented driver of burnout, and protecting clinical staff from routine overnight calls is a retention strategy. An outsourced service absorbs that load without adding headcount to an already tight hiring environment.
Clinical quality is where the comparison often tips. In-house nurses working occasional on-call shifts may handle calls inconsistently. Our nurses follow Schmitt-Thompson clinical protocols on every call, regardless of volume or time of night.
Before finalizing your evaluation, consider how each model performs across these dimensions:
- Clinical consistency: Validated protocols applied at 2 a.m. on a holiday, not just during peak hours.
- Cost structure: Per-call or monthly pricing replaces unpredictable overtime and scheduling costs.
- Staff protection: Removing routine after-hours calls directly reduces burnout pressure.
- Scalability: A flu surge does not require emergency staffing calls when volume is handled externally.
- Hiring dependency: In-house after-hours teams require nurses you may not be able to recruit in a shrinking workforce.
Our guide on medical message automation to improve after-hours message accuracy walks through the operational questions worth asking before committing to either model.
Frequently Asked Questions
What is an after-hours medical answering service?
An after-hours medical answering service handles patient calls when a clinic or practice is closed. The strongest versions staff licensed RNs who use clinical protocols to assess symptoms and direct patients to the right level of care, rather than simply taking messages.
How is RN triage different from a standard medical answering service?
A standard answering service logs and relays messages. An RN triage service has a licensed nurse evaluate symptoms and assign acuity. The nurse then routes the patient appropriately – whether that means home monitoring, a next-day appointment, or the ER.
What are Schmitt-Thompson protocols and why do they matter?
Schmitt-Thompson protocols are evidence-based clinical guidelines developed for telephone triage. They standardize how nurses evaluate symptoms by phone, reducing variability and supporting safe, consistent clinical decisions across thousands of calls.
What does URAC accreditation mean for a nurse triage service?
URAC Health Contact Center accreditation means the service has met independently audited standards for clinical staff qualifications, response times, HIPAA-compliant documentation, and triage call handling. Buyers get a verifiable quality benchmark rather than a self-reported claim.
Can outsourced nurse triage actually reduce unnecessary ER visits?
Yes. According to a systematic review published in The Effects of Telephone Consultation and Triage on Healthcare Use and Patient Satisfaction, 50% or more of after-hours calls can be fully resolved by phone without any in-person visit. Our nurses return calls in about 9 minutes on average, well within the URAC 30-minute standard. Roughly 1 in 6 triage calls avoids an unnecessary ER visit.
Closing Thoughts
The gap between a message-relay service and a nurse triage service is not a vendor preference. Picture a scared parent at midnight. One service tells her to drive to the ER. The other gives her clinical guidance that keeps her family home and safe. Those are two very different outcomes.
Ask concrete questions. Start with who answers the call. Then ask what protocols govern the conversation, how quickly that happens, and who is accountable when something goes wrong.
We answer each of those questions with specifics. Our nurses follow physician-approved Schmitt-Thompson protocols and operate within a URAC-accredited, physician-led structure built on nearly two decades of experience.
If your organization is ready to close the after-hours gap, the Nurse Triage On Call guide walks through exactly how a structured triage program works in practice. You can also schedule a conversation with our team to discuss your specific coverage needs.
Sources
- After-Hours Care and its Coordination with Primary Care in the U.S.
- The impact of urgent care centers on nonemergent emergency department visits (2021)
- NCQA
- How Many ED Visits Could be Managed at Urgent Care Centers and Retail Clinics?
- American Medical Association (2026)
- American Medical Association (2025)
- HRSA Bureau of Health Workforce
- The effects of telephone consultation and triage on healthcare use and patient satisfaction: a systematic review
- The Journal for Nurse Practitioners (2015)
- URAC